Written by Dr. Daniel Fraser (MBBS, FRACP) – Physician
Question 1
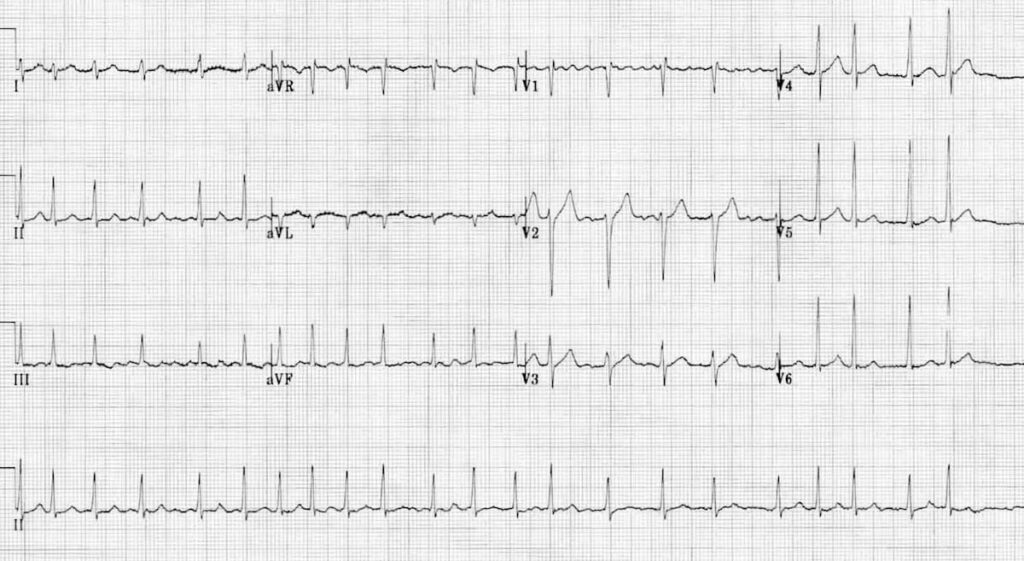
A 56-year-old man presents to the emergency department with complaints of chest pain and lightheadedness. On examination he has a blood pressure of 85/50 mmHg, rapid and barely perceptible pulse of 160 bpm and respiratory rate of 24 breaths per minute. An ECG is obtained which is shown in the accompanying photograph. Which one of the following is the most appropriate next step in management?
A) Atropine
B) Intravenous diltiazem
C) Intravenous metoprolol
D) Pace maker insertion
E) DC cardioversion
Question 2
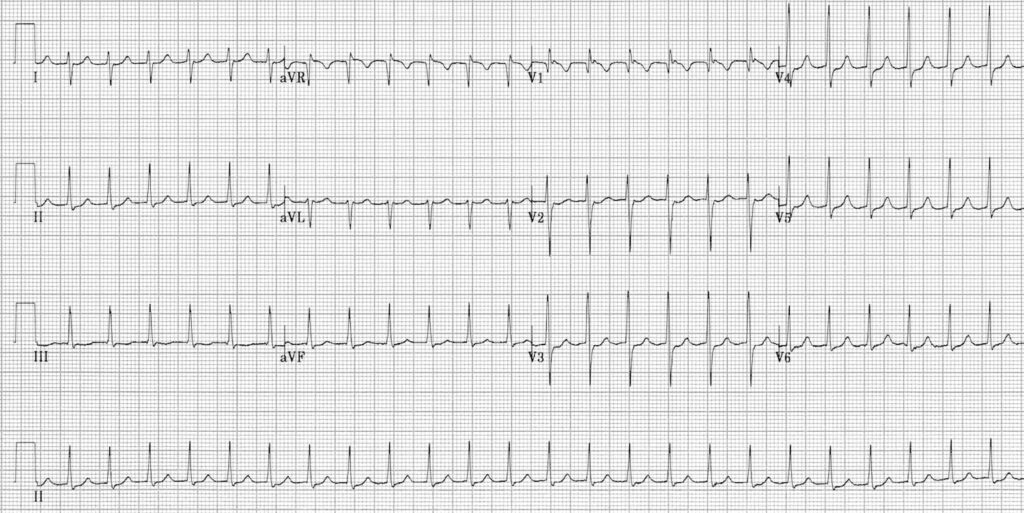
A 72-year-old woman presents to the clinic with complaints of intermittent palpitations and mild shortness of breath over the past month. She denies chest pain or syncope. On examination, her pulse is irregularly irregular with a rate of about 110 bpm. Blood pressure is 130/80 mmHg. An ECG is obtained as is as follows;
Which one of the following is the most likely diagnosis?
A) Atrial flutter
B) Atrial fibrillation
C) Sinus tachycardia
D) Ventricular tachycardia
E) Supraventricular tachycardia
Question 3
A 60-year-old man presents to the Emergency Department with palpitations for the past 2 weeks. On examination, his blood pressure is 125/95 mmHg and his heart rate is irregular at 160 bpm. An ECG shows atrial fibrillation (AF). He is started on metoprolol for rate control, and electrical cardioversion is planned. Which one of the following should be used for anticoagulation?
A) Heparin, 24 hours before the procedure
B) Warfarin 4 weeks before, to 4 weeks after the procedure
C) Aspirin
D) Apixaban from 48 hours before, to 48 hours after the procedure
E) Flecainide