Written by Dr. Daniel Fraser (MBBS, FRACP) – Physician
Question 1
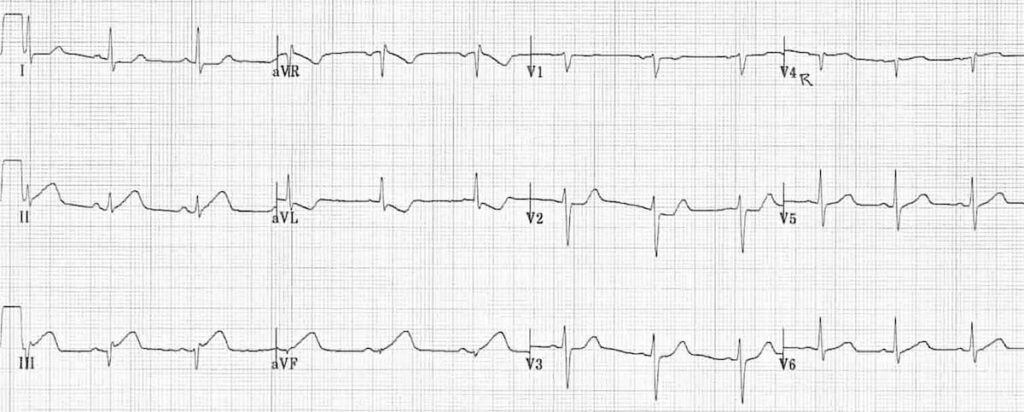
A 65-year-old man presents to the Emergency Department with complaint of chest pain radiating to his jaw for the past 2 hours. The patient is given aspirin, sublingual nitroglycerine (TNG), and supplemental oxygen. With these measures the chest pain subsides. An ECG is obtained and is as follows. A troponin level is requested with the result still pending. Which one of the following is the next best step in management?
A) Send the patient home on aspirin
B) Coronary angiogram and angioplasty
C) Thrombolysis
D) Admit and wait for the troponin results
E) Perform stress test
Question 2
A 62-year-old man presents to your clinic for a follow-up visit. He had a myocardial infarction (MI) 4 years ago. He is currently on aspirin 80 mg daily. He follows a healthy diet and does exercise regularly. Laboratory studies are all within normal parameters. An ECG is obtained that is normal. Which one of the following is the most appropriate advice for him?
A) Reinforce the importance of a healthy diet and regular exercise
B) Stop aspirin
C) Add statins
D) Tell him he does not need any further follow-up
E) Add warfarin
Question 3
A 72-year-old woman is brought to the Emergency Department with chest pain of several hours duration. Of physical findings on examination, a blood pressure of 98/50 mmHg and an irregular pulse of 120 bpm are remarkable. An ECG shows ST elevation in leads V2 and V4. Which one of the following will be the most appropriate initial management option?
A) Cardioversion
B) Thrombolysis with TPA
C) Lidocaine
D) Verapamil
E) Digoxin