Question 1
A 25-year-old man presents to the emergency department after falling on his outstretched left arm while playing rugby. He complains of severe pain in his left shoulder and inability to move the arm. On examination, the left shoulder appears flattened anteriorly with a prominent acromion, and the patient holds his arm slightly abducted and externally rotated. There is tenderness over the shoulder joint and limited range of motion due to pain. An X-ray of the left shoulder (see image) is performed.

Which of the following is the most likely diagnosis?
A) Left rotator cuff tear
B) Left anterior shoulder dislocation
C) Left clavicle fracture
D) Left proximal humerus fracture
E) Left posterior shoulder dislocation
Question 2
A 32-year-old man is brought to the emergency department after a seizure. He complains of pain and limited movement in his left shoulder. On examination, the shoulder appears held in internal rotation with limited external rotation and anterior fullness is absent. There is tenderness over the posterior shoulder region. An X-ray of the left shoulder (see image) is performed.
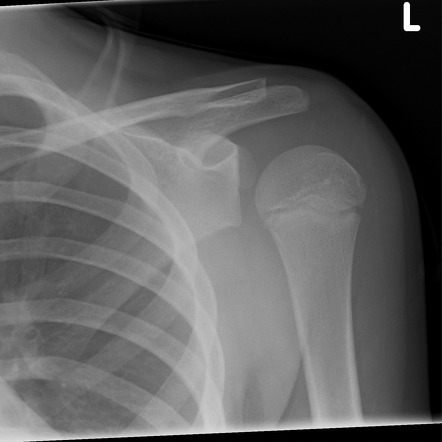
Which of the following is the most likely diagnosis?
A) Right anterior shoulder dislocation
B) Right posterior shoulder dislocation
C) Right clavicle fracture
D) Right proximal humerus fracture
E) Rotator cuff tear
Answer: B) Right posterior shoulder dislocation
Explanation:
History and Clinical Examination:
Posterior shoulder dislocations are uncommon and often occur after seizures, electric shocks, or direct trauma. Patients present with shoulder pain, limited range of motion, especially restricted external rotation, and the arm is usually held in internal rotation and adduction. Unlike anterior dislocations, there is no anterior shoulder fullness or visible deformity. Tenderness may be noted over the posterior shoulder.
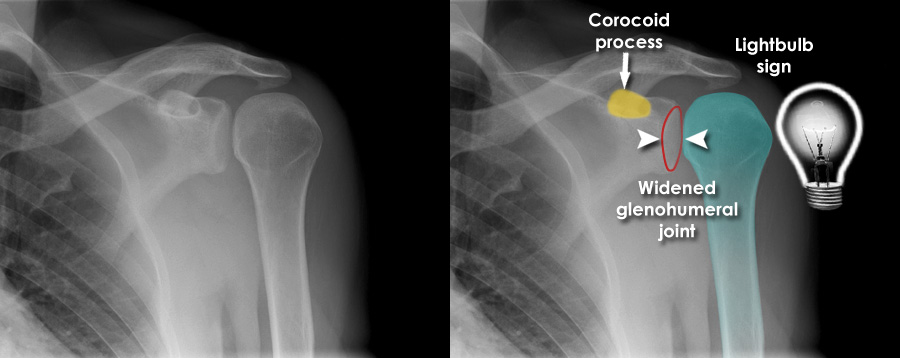
X-ray Features:
Posterior dislocations can be subtle on standard anteroposterior (AP) X-rays. The humeral head appears displaced posteriorly relative to the glenoid fossa. Classic signs include the “light bulb sign” (rounded humeral head due to internal rotation), and “rim sign” (widening of the glenohumeral joint space). Additional views such as axillary or scapular Y view are critical for diagnosis.
Management:
Early diagnosis and prompt closed reduction under sedation are important to avoid complications such as chronic instability and arthritis. Immobilization followed by rehabilitation is recommended after successful reduction.
Question 3
A 22-year-old rugby player presents to the emergency department after falling directly onto his right shoulder during a match. He complains of pain and swelling over the top of the shoulder and difficulty lifting his arm. On examination, there is tenderness and swelling localized over the acromioclavicular joint, with a noticeable bump over the lateral end of the clavicle. The cross-arm test reproduces pain. An X-ray of the right shoulder (see image) is obtained.

Which of the following is the most likely diagnosis?
A) Clavicle fracture
B) Acromioclavicular (AC) joint separation
C) Rotator cuff tear
D) Glenohumeral dislocation
E) Proximal humerus fracture